FDA and EMA accept regulatory applications for Boehringer Ingelheim's Gilotrif for treatment of advanced SCC of the lung
Boehringer Ingelheim has announced that both FDA and EMA have accepted filing applications for afatinib for the treatment of patients with advanced squamous cell carcinoma (SCC) of the lung progressing after treatment with first-line chemotherapy. Afatinib has also been granted orphan drug designation by the FDA — a status given to a product intended for the treatment of a rare disease or condition.
Dr Jörg Barth, Corporate Senior Vice President, Therapy Area Head Oncology, Boehringer Ingelheim commented: "Working with the US and EU regulatory authorities marks the next stage in our journey to hopefully provide patients with a new, oral treatment for squamous cell carcinoma of the lung, a condition with an extremely poor prognosis. This is an encouraging prospect for Boehringer Ingelheim, as we remain fully dedicated to improving and extending the lives of patients with different types of lung cancer."
The submissions are based on data from the Phase III LUX-Lung 8 trial that compared Gilotrif(®) (afatinib) to Tarceva (erlotinib) in patients with advanced SCC of the lung progressing after treatment with first-line platinum-based chemotherapy. Data from the trial showed that treatment with afatinib resulted in superior progression-free survival (PFS, primary endpoint), reducing the risk of cancer progression by 19%, and superior overall survival (OS, key secondary endpoint), reducing the risk of death by 19% compared to erlotinib in this patient population.
In the LUX-Lung 8 trial, an improvement in quality of life and control of cancer symptoms was observed with afatinib versus erlotinib. More patients had improved overall health-related quality-of-life with afatinib than with erlotinib (36% vs. 28%). Significantly more patients had an improvement in cough with afatinib than with erlotinib (43% vs. 35%). Differences in the proportion of patients with improved dyspnea (51% vs. 44%) and pain (40% vs. 39%) were not significant for afatinib versus erlotinib. Afatinib significantly delayed time to deterioration of dyspnea compared with erlotinib. Time to deterioration of both pain and cough was similar for afatinib versus erlotinib.
The rate of severe adverse events was similar between the two treatment arms with differences observed in the incidence of certain side effects. A higher incidence of severe diarrhea and stomatitis (mouth sores) was observed with afatinib compared to erlotinib (grade 3 diarrhea: 10% vs. 2%; grade 3 stomatitis: 4% vs. 0%), while a higher incidence of severe rash/acne was reported with erlotinib compared to afatinib (grade 3 rash/acne: 10% vs. 6%).
Related News
-

News The next 15 drugs up for negotiation with Medicare include several blockbusters
By now, everyone is quite familiar with the drug price negotiations taking place between drug companies and the Centres for Medicare & Medicaid Services (CMS) in the USA as part of measures being taken to reduce the cost of drugs for patients, to make ... -

News PSCI Welcomes Delpharm, Samsung Biologics, and Suven as First Supplier Partners
The pharmaceutical industry continues to evolve with an increasing focus on responsible sourcing, sustainability, and collaboration across the supply chain. Under a new model to recognise suppliers within the pharmaceutical and healthcare industry that... -

News Drug prices agreed upon as part of the US Inflation Reduction Act
The Inflation Reduction Act brought into constitution by the Biden administation in 2022, which proposed a drug price negotiation between the government and pharmaceutical companies, has reached it's first agreement. -
.png)
News Eisai Alzheimer’s drug authorised in UK but still faces obstacles
In partnership with BioArctic AB, pharmaceutical company Eisai has been granted Marketing Authorisation by the Medicines and Healthcare products Regulatory Agency (MHRA) for its Alzheimer’s disease drug product Leqembi. -
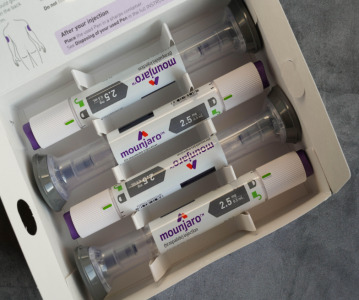
News Eli Lilly's weight loss drugs removed from the FDA's shortage list
The US FDA have recently updated their drug shortage list. The recently released list shows that all dosage forms of Eli Lilly's weight-loss drug Zepbound and their diabetes drug Mounjaro are now available. -

News Global advancements in the diagnosis and treatment of rare diseases: Rare Disease Day 2024
Rare Diseases Day is celebrated on the 29th February 2024 and represents the plight of rare disease patients to gain diagnosis and access to suitable treatment. -
News Pharmaceutical industry supports COP28 health stance in joint statement
As COP28 takes place over this week in Dubai, UAE, several bodies in the pharmaceutical and health industries have come together to announce support of key movements in sustainability in the sector, and to recognise sustainability as a health issue.&nb... -

News Biden backs Cold-War measures to shore-up medical supply chains
In a recent strategy to combat rising inflation and the cost of living crisis, President Joe Biden has invoked a Cold War-era act to increase investment in a selection of medicines and supplies.
Recently Visited
Position your company at the heart of the global Pharma industry with a CPHI Online membership
-
Your products and solutions visible to thousands of visitors within the largest Pharma marketplace
-
Generate high-quality, engaged leads for your business, all year round
-
Promote your business as the industry’s thought-leader by hosting your reports, brochures and videos within your profile
-
Your company’s profile boosted at all participating CPHI events
-
An easy-to-use platform with a detailed dashboard showing your leads and performance